Lyme disease is the most common tickborne infection in Chicago, caused by the bacterium Borrelia burgdorferi and rarely, Borrelia mayonii.
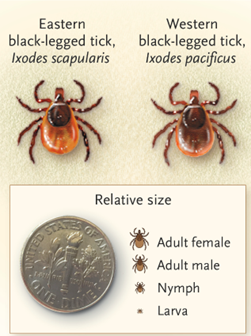
Lyme is transmitted to humans through the bite of black-legged ticks (also known as deer ticks in the eastern United States) and western black-legged ticks in western United States infected with the bacterium Borrelia (Figure 1).
Approximately 20 % of infected patients recall tick bites.
Infection occurs at least 36 - 48 hours after tick attachment.
The incubation period is 3-30 days after the tick bite.
The primary reservoir and host for the bacteria: Small rodents, including the white-footed mouse (Figure 2).
Host for ticks: Whitetail deer (Figure 3).
Figure 1: Common Ticks Associated with Lyme Disease in North America.
Lyme disease has three stages, each with different clinical manifestations. Without appropriate antibiotic treatment, disease can progress from stage 1 to stage 2 or 3 within weeks or months.
Stage 1 occurs 3 to 30 days after a tick bite and usually consists of Erythema Migrans (EM), a slowly expanding skin lesion, accompanied by flulike symptoms (fever, headache, tiredness, swollen lymph nodes, and joint and muscle pain). EM occurs in 70-80% of infected people and typically, but not always, appears like a bull’s eye or target appearance (Figure 4).
Stage 2 (or early dissemination infection stage) occurs weeks later. In this stage the manifestations may include multiple EM rashes distant from the site of tick bite (Figure 5) and neurologic symptoms including aseptic meningitis (typically with a lymphocytic pleocytosis), cranial neuritis (including Bell’s Palsy), or encephalitis. Another early disseminated form of disease is Lyme carditis which may include second-degree and third-degree heart blocks or myopericarditis.
Stage 3 (late dissemination infection stage) usually occurs months after a tick bite. This stage is commonly associated with intermittent or persistent arthritis in one or a few joints, most commonly the knees, over a period of several years.
When assessing a patient for Lyme disease, healthcare providers should consider:
The signs and symptoms of Lyme disease
The likelihood that the patient has been exposed to infected blacklegged ticks.
The possibility that other illnesses may cause similar symptoms.
Results of laboratory tests, when indicated.
CDC currently recommends a two-step testing process for Lyme disease. Both steps are required and can be performed on the same blood sample. Serologic testing should use validated first- and second tier tests (Figure 6):
Standard two-tier test (STTT): An initial (first tier) positive or equivocal enzyme immunoassay (EIA) or immunofluorescent assay (IFA) followed by a second positive Immunoglobulin M (IgM) or Immunoglobulin G (IgG) western immunoblot (WB).
Modified two-tier test (MTTT): An initial (first tier) positive or equivocal enzyme immunoassay (EIA) or immunofluorescent assay (IFA) followed by a second positive IgM or IgG enzyme immunoassay (EIA).
If the first step in testing is negative, no further testing is recommended.
If the first step is positive or equivocal/indeterminate, the second step should be performed.
The overall result is positive only when the first test is positive or equivocal and the second test is positive.
Other methods for diagnosis:
Culture for B. burgdorferi or B. mayonii
PCR for B. burgdorferi or B. mayonii
Immunohistochemical assay (IHC)
Key points to remember:
Most Lyme disease tests are designed to detect antibodies made by the body in response to infection.
Antibodies can take several weeks to develop, so patients may test negative if infected only recently.
Antibodies normally persist in the blood for months or even years after the infection is gone; therefore, the test cannot be used to determine a cure.
Infection with other diseases, including some tickborne diseases, or some viral, bacterial, or autoimmune diseases, can result in false positive test results.
Some tests give results for two types of antibodies, IgM and IgG. Positive IgM results should be disregarded if the patient has been ill for more than 30 days.
Figure 6:
Figure 6. Standard 2-tier and modified 2-tier algorithms for serodiagnosis of Lyme disease. The US Centers for Disease Control and Prevention recommended a standard 2-tier algorithm (A) and the modified 2-tier algorithm (B).
*For patients with signs or symptoms consistent with Lyme disease for less than 30 days, the provider may treat and follow up with a convalescent- phase serum sample. Patients with erythema migrans should receive treatment of the bases of clinical diagnosis. WB: Western blot. (2)
Antimicrobial prophylaxis for the prevention of Lyme disease following a tick bite might be beneficial in certain high-risk criteria. Which include 1) an ixodes spp vector, 2) bite occurred in a highly endemic area and 3) the tick was attached for ≥36hours. (Lyme-pep-low-ink-p.pdf (cdc.gov)) (9)
In the early infection, appropriate oral antibiotic treatment (usually doxycycline, twice daily; or Amoxicillin or Cefuroxime for 14 – 21 days are successful options depending on person’s age, medical history, pregnancy status or allergies. (Clinical Care of Lyme Disease | Lyme Disease | CDC).
For some individuals with neurologic, cardiac, or arthritis, intravenous antibiotics treatment (often ceftriaxone) for 28 days may be necessary.
Disease Prevention
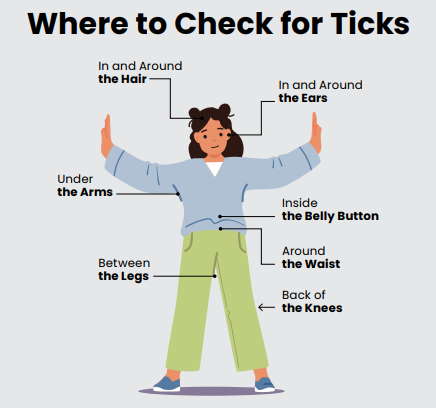
Steps to prevent Lyme disease include using insect repellent, checking the body after being outdoors (figure 7), removing ticks promptly, applying pesticides, and reducing tick habitat.
1.Use fine-tipped tweezers to grasp the tick as close to the skin as you can.
2.Pull upward with steady, even pressure. Don’t twist or jerk the tick.
3.After removing the tick, clean the bite area and your hands with rubbing alcohol or soap and water.
4.Dispose of the tick by flushing it down the toilet. If you would like to bring the tick to your healthcare provider for identification, put it in rubbing alcohol or place it in a sealed bag/container.